This is a 63 year old woman with VA of 20/60 and NLP with poorly controlled DM and lost to follow-up for 2 years. What are the FA findings, and what can you infer as to the cause of her blindness in the left eye?


Short answer (annotated images to follow):
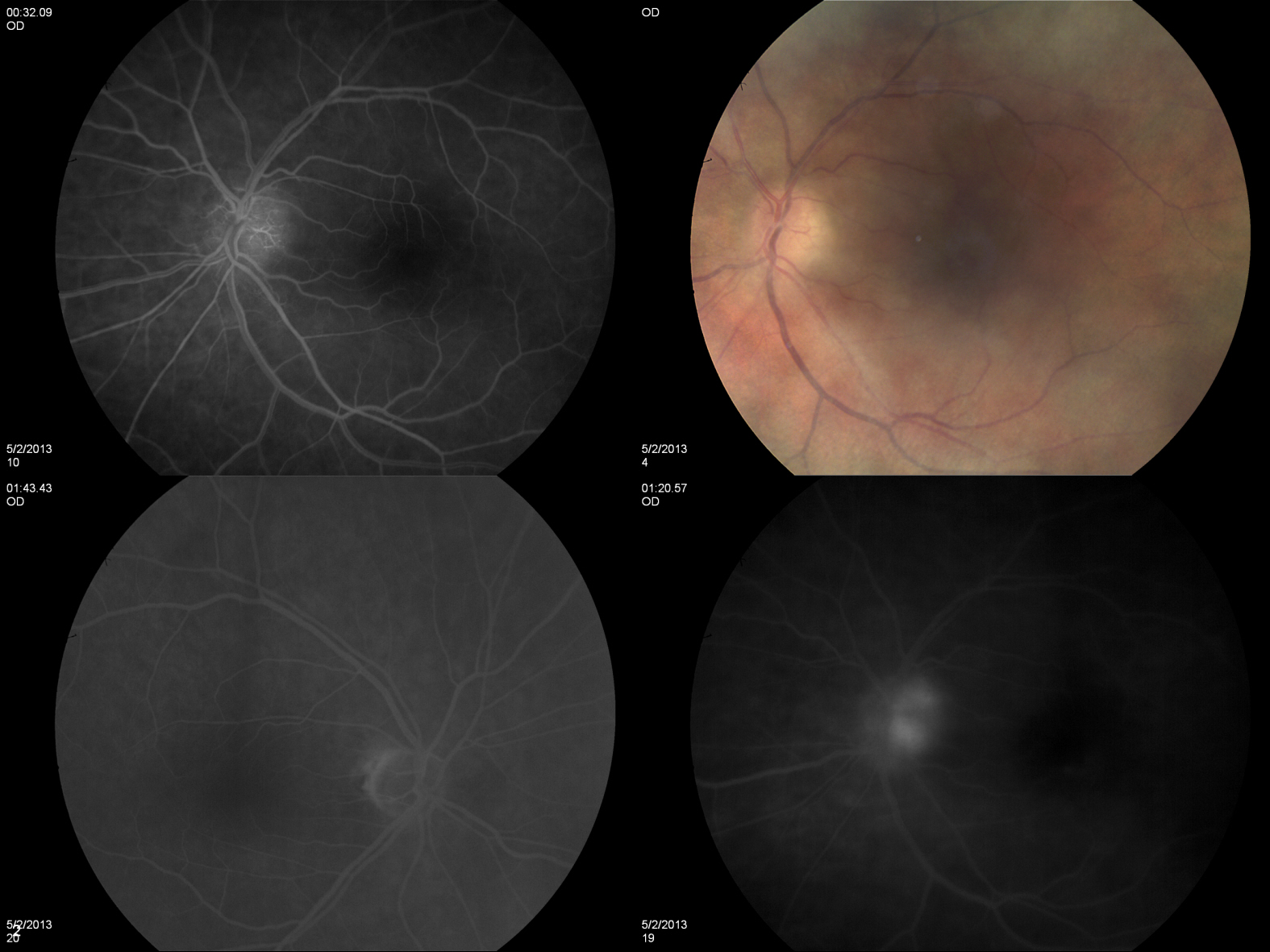
The first image demonstrates a right eye in a patient with PDR. Large areas of non-perfusion can be seen, with adjacent NVE (remember, neovascularization is often found on the border of perfused and non-perfused tissue). The 2nd image is an anterior FA which demonstrates NVI (along with PCIOL, superior iridotomy). The natural progression of NVI, which can often be seen first at the pupilary border, eventually causes fibrovascular obstruction of the trabecular meshwork, results in neovascular glaucoma. We can infer that the fellow eye has long since suffered glaucomatous damage to the optic nerve 2/2 NVI, thus resulting in the NLP visual acuity.